What is the problem?
To Err is Human. This is how a landmark paper from 2000 starts, recognizing that “the problem is not bad people in health care–it is that good people are working in bad systems that need to be made safer“*. The consequences of errors can be described by adverse events. Adverse events that are related to medication and or drug/fluid incidents constitute about 20% of all types of adverse events, which makes this the second most common type of adverse event†.
The medication/order cycle
The use of medication (or any therapeutic order) is a cyclic process:
- According to product info and dosing rules
- A prescription is created which
- Has to be validated
- Planned and
- Prepared
- The administration has to be recorded and
- Finally the effects have to be evaluated to determine subsequent alterations and/or additional prescriptions
A prescription is initiated by an indication. Once the indication is established, all subsequent steps are protocolized. According to the indication a suitable therapy is chosen and, given patient specifics, the route, dose, timing etc.., all can be found in specific protocols and/or drug formularies. Therefore, two mental processes are required:
- Looking things up (right drug, dose, route, dose, etc..)
- Calculating the numbers (total dose, infusion rate, concentration, etc..)
The problem is, people are particularly bad at both those two tasks. However, computers can perform these types of jobs at extreme speed, without any mistakes and can do so tirelessly, 24 hours a day, seven days a week.
The Treatment Plan
When a prescription is generated, this is in fact added to a set of running prescriptions, i.e. the treatment plan. Therefore, during the prescribing process, the running prescriptions have to be taken into account:
- Interactions: A prescription has to be checked against running prescriptions whether this would cause an unwanted interaction.
- Dubble medication: A prescription could be already be prescribed by a different drug.
- Totals calculations: When adding a prescription to a treatment plan, calculation of totals are involved, as explained below.
The totals calculations in particular pose a challenge in the prescription process. For example, the total fluid intake is for obvious reasons extremely important and has to be calculated by adding up all prescribed fluid drugs, other fluids and feeding. However, this not only applies to total fluid intake, but also to elektrolytes, nutrients, and any other relevant substance. In fact this means that indirectly, these parameters are prescribed and have to be ‘dosed’ as well.
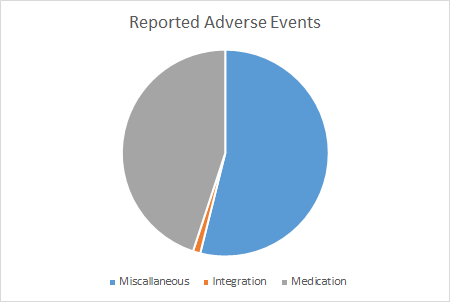
Adverse events related to medication, fluids an feeding
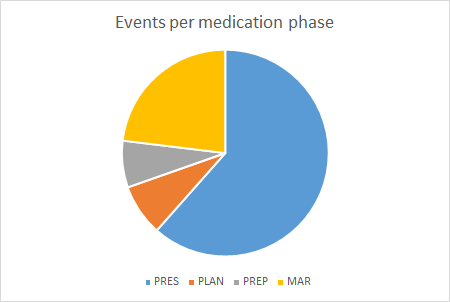
In a recent in hospital analysis (University Medical Center Utrecht, Wilhelmina Children’s Hospital), we found that almost 50% of reported incidents where medication and/or fluid related.
Of these incidents, more than a 60% could be traced down to prescription errors.
So, there is a clear and present medical problem, reportedly covered in literature with a high incidence that could be solved (easily?) by computers. But recent literature still mentions high incidences of prescription errors, especially in pediatrics‡.
What is GenPRES?
Goals
GenPRES is a Computerized Provider Order Entry (CPOE) system that aims to
- Prevent all prescription errors related to finding the required information and performing all necessary calculations to create prescriptions
- Support the subsequent phases in the medication process:
- Validation
- Planning
- Preparation
- Recording and
- Evaluation
- And, thus, eliminate virtually all (preventable) errors related to medication fluids and feeding while at the same time enhance the efficiency of the involved workflow.
The central theme around which the system is build is:
Safe by Default
Once the indication for prescribing for a specific patient is clear, the system will support all subsequent steps in the medication cycle such that the prescriber doesn’t have to look up the required information and/or perform any calculations. This will be provided by GenPRES for all the phases in the medication process. Safety is guaranteed because the system will not make mistakes by accidentally reading the wrong information and/or in performing calculations. Sticking to defaults (i.e. protocols) also ensures an efficient workflow.
It is important to realize that not only the different phases in the medication cycle have to be supported, but also there are different stake holders (fig 1.):
- Pharmacists. Managing the available medication products, creating protocols an formularies and often have an important role in validating drug prescriptions.
- Prescribers. Physians and other health care providers that prescribe, validate and evaluate drug therapy.
- Nursing staff. Planning, preparing and administering the medication.
- And finally, but most importantly, the patients receiving the prescribed medication, fluids and feeding.
The different phases and stakeholders require different information for essential an identical prescription.
For example:
- Prescribers:
- Dopamine iv 5 mcg/kg/min
- Paracetamol rectally 70 mg/kg/dag in 3 x /day
- Pharmacists:
- DOPAMINE 40 MG/ML AMPULE 5ML
- PARACETAMOL 120 MG SUPP
- Nursing staff:
- Dopamine 5 ml in 45 ml NaCl 0,9%, 1 ml/hour
- Paracetamol supp 08:00, 14:00 en 22:00 hour
A prescriber is interested in the route, frequency and therapeutic dose. A pharmacist is interested in which products are used and have to be dispensed. Nursing staff require the exact product quantities, infusion rates and planning of medication administration. Therefore, a prescription has different viewpoints, that have to be modelled and calculated accordingly.
Optimized
Efficient
Alternatives to GenPRES?
Most hospitals with an Electronic Health Record System (EHRS) nowadays also employ Computerized Prescription Order Entry (CPOE). These CPOE systems currently are limited to prescribing medication with limited decision support.
In fact, the above mentioned adverse events (fig. 2) where extracted from a hospital registry in which a vendor based CPOE is used with incomplete decision support.
There currently are simply no alternatives available that fulfil all the requirements to prevent medication related adverse events, other than GenPRES.
Why GenPRES?
There are a number of compelling reasons to develop and use a CPOE like GenPRES.
1. Preventable adverse events should be prevented
Prescription errors due to deficient information and/or errors in calculations can/should entirely be prevented.
2. Prescriptions should be generalized
Prescriptions can be generalised to other therapeutic orders like:
- Fluids (enteral and intravenous)
- Feeding (enteral and intravenous)
- Related laboratory orders
3. A CPOE should support all phases of the Medication Cycle
GenPRES is specifically modeled to support all subsequent phases in the ‘Medication Cycle’
GenPRES is designed to be used on a Pediatric Intensive Care Unit (PICU). In a PICU you can find the broadest possible range of patients, from birth (about 2 kg) up to 18 years (sometimes with weights > 100 kg). So, there is an extreme variation of prescription scenarios that all have to be supported. In other words, if it works on a PICU, it will work in most (if not all) other clinical and non-clinical settings.
In fact, the efficiency in preventing prescription errors by providing decision support has been demonstrated in a recent study that detected only 2 preventable protocol deviations in dosing per 1000 prescriptions§.
Conclusion
GenPRES is designed to prevent errors while at the same time increase efficiency of workflow for every stage in the Medication Cycle. This will increase patient safety, improve efficiency and, thus, lower the overall costs of healthcare.
- *Institute of Medicine (US) Committee on Quality of Health Care in America. To Err is Human: Building a Safer Health System. Kohn LT, Corrigan JM, Donaldson MS, editors. Washington (DC): National Academies Press (US); 2000. PMID: 25077248.
- †Schwendimann R, Blatter C, Dhaini S, Simon M, Ausserhofer D. The occurrence, types, consequences and preventability of in-hospital adverse events – a scoping review. BMC Health Serv Res. 2018 Jul 4;18(1):521. doi: 10.1186/s12913-018-3335-z. PMID: 29973258; PMCID: PMC6032777.
- ‡Brennan-Bourdon LM, Vázquez-Alvarez AO, Gallegos-Llamas J, Koninckx-Cañada M, Marco-Garbayo JL, Huerta-Olvera SG. A study of medication errors during the prescription stage in the pediatric critical care services of a secondary-tertiary level public hospital. BMC Pediatr. 2020 Dec 5;20(1):549. doi: 10.1186/s12887-020-02442-w. PMID: 33278900; PMCID: PMC7718655.
- §Fatema Hashemi, Yves Liem, Thomas G. Gelder, Toine C.G. Egberts, Casper W. Bollen, A Clinical Decision Support System Can Effectively Prevent Dosing Errors. European Society of Pediatric and Neonatal Intensive Care Congress 2021.